
1. Rationale for the research
1.1 The mental health needs of adolescents and young adults (both those with SMI and those with more common conditions) are distinct from those of children and adults. SCIE reported that ‘difficulties in providing good support during mental health service transitions are linked to broader issues in providing effective, age-appropriate, accessible mental health support to young people. The way in which CAMHS and AMHS are organised does not always fit easily with the ways in which mental health problems are experienced by young people’. We know that young people with MH needs who are either untreated or not supported tend to have poor MH and other outcomes in adulthood; for e.g. There is a strong causal link between untreated ADHD and violent crime in young adulthood. We also know that some young adults with mental health needs will have complex co exiting medical, educational and social needs also.
1.2 Based on the literature review and interviews HWL have carried out with a number of local stakeholders we have identified some particular areas of focus, which would be of most benefit to local commissioners and services in understanding the experiences of young adults in transition and where improvements could be made and good practice built upon.
1.3 Some young people might find themselves without the support they need, whether it secondary, primary or voluntary sector due to:-
- Different referral and/or eligibility criteria between CAMHS and adult services.
- Inconsistencies in age cut-off points, with some services ending when a young person is 16 yrs – with adult secondary (and some primary) care services being typically for 18 yr olds and over.
- young adults with learning disabilities, ASD, ADHD etc will have ongoing, specialist support needs - but there are limited specialist adult services for them.
1.4 Where ‘transition’ does take place this may still lead to poor experience and outcomes due to:-
- Gaps in services due to lack of age appropriate and accessible services
- Impact of the ‘shift’ from a more supported approach (in young people’s services) to a model that relies on greater self-motivation and independence.
- Frequently inconsistent and poor practice.
- Inflexible and unresponsive services.
- Lack of understanding of young people's mental health problems.
- Lack of supporting development of resilience in young people.
- Significant differences in types, levels and access criteria for services in different areas.
1.5 Young adults and carers have identified changes which could be made to help overcome barriers and lead to ‘better’ transitions:
- Services and pathways which cross the service transition period of 16-18 yrs, e.g. provide services up to the age of c 25 yrs.
- Flexible services without strict 'cut-off' points- especially for young people with emotional problems, complex needs, mild learning disability, ADHD and ASDs, where there are limited statutory adult services beyond GPs.
- Link between services – e.g. through peer supporters who stay with them for a time.
- More and better support from GPs/primary care.
- Support geared for younger adults.
1.6 Little systematic work has been done in Lambeth to explore the experiences and outcomes for different groups of younger adults who are about to/in the process of, or have transitioned from children’s services. ‘The Young Lambeth Emotional Wellbeing and Mental Health Strategy and Plan 2015 – 2020 identified some priorities for improving the transition of young people with mental health needs to adulthood. These included:
- Review current transition protocols from CAMHS to AMH and ensure compliance across the system.
- Establish a specific work stream to develop transition services for those exiting CAMHs to be initiated, incorporating service user experience and looking at innovative ways to delivery.
- Work with adult services to ensure alignment of overlapping services for young adults, 18+, and to identify alternative and innovative models to meet the needs of those likely to transition to adult services.
1.7 This research will help to explore the extent to which these priorities have improved experience and outcomes for young people.
2. Research focus
2.1 There is a wide diversity of mental health needs, often coexisting with educational, medical and social needs of this broad group of young people, which are likely to require often significantly different approaches and interventions, ranging from very complex cases with involvement of multiple services to those requiring a single service intervention in primary care. For example, not every young person in CAMHS will need to transfer to adult MH services as many will not have ‘severe and enduring’ MH needs. However, transition to alternative support non secondary care services such as voluntary sector services, primary health care and other universal services, remains important.
2.2 Based on our scoping work our null hypotheses are that:
- Many individuals who require support ‘drop out’ of the system at age c 18 yrs.
- Some individuals with enduring mental health issues do not access adult mental health, but continue to access support and strategies established earlier with CAMHS or other agencies, often using non specialist forms of support.
- Some individuals who required support, will cease to need this as other areas of their lives, e.g. employment/education, relationships, living arrangements (i.e. leaving the familial home) change
- Many individuals who require support and are linked to adult services, do not get the type and quality of the support they need, either in secondary or primary care.
- Where individuals do not get the right support they are more likely to risk poorer health and wellbeing outcomes during adulthood.
- Some particular groups experience poorer outcomes from transition, e.g. care leavers.
2.3 To help reflect this diversity, in the design and delivery of the research we will purposively explore issue related to disability, social class, gender, sexuality, language and ethnicity as these are likely to have a significant bearing on experiences and outcomes.
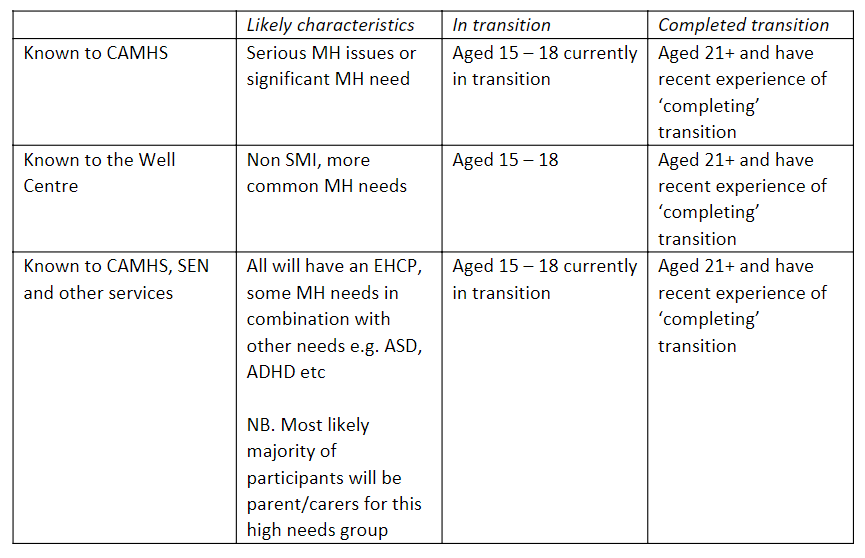
2.4 Taking these characteristics into account and in order to provide a clear focus for the research, will focus on three key cohorts:
- Young people with a diagnosed serious mental health issues, who are likely to be known to CAMHS and likely to meet the criteria for Adult Mental Health Services, including both those that transition to AMHS and those who ‘drop out’ of services.
- Young people with identified more common mental health needs such as anxiety, self- harming, depression, emerging personality disorders etc. Some of this group are likely to be known to CAMHS, others will have received support through the Well Centre.
- Young people with Education and Health Care Plans, who have co existing learning disabilities, ASD, ADHD etc. This group are likely to be known to a CAMHS team, have an SEN coordinator and often an allocated social worker.
3. Methodology
3.1 As the primary aim of the research is to discover young people’s experiences and the methods will include a number of depth qualitative interviews with young people (and where appropriate their carers) for members of each of the cohorts above.
3.2 What we will be talking to young people about:
- Experience of preparation for adulthood
- Experience of move to adult life/services/support
- What does and what could help with transition (e.g. Peer Support)
- The experience of transition – moving from a highly supportive environment to a more independence focused one.
- What other issues adversely impact on their ability to stay mentally well? e.g. stigma, social isolation, housing, relationships with family, economic independence, physical health etc.
- How do people find their own help?
- How can we build resilience in individuals better?
- What early help in the community, through informal and formal networks would be helpful to individuals?, etc.
- What does ‘good’ look like and feel like for young adults in relation to service design and delivery, (including examples of good practice?
3.3 Which young people we will be talking to:
We aim to achieve completed individual interviews with up to 5 young people (or their carers; N=30) in each of the six groups above in addition to the on line questionnaire and focus group participation.
3.4 How we will be talking to them?
HWL preferred approach to undertaking field work for this research would be face to face interviews supplemented by focus groups at key stages of the research and some self-complete on line questionnaire designed to help triangulate findings and also. As this is not feasible at this time we will instead offer some alternatives to people who wish to participate, these will include, face to face zoom meetings, telephone interviews and webinar focus groups. These options acknowledge that individuals would have different preferences of interaction.
3.4.1 Semi structured interviews via zoom
Participants will be offered a zoom interview. This would be conducted by two HWL volunteers or staff, one will lead the interview while the other will take notes. All participants will be given the choice of being accompanied during the session by a friend or supporter if they wish.
3.4.2 Telephone interviews
These will be offered to individuals who wish to participate but cannot access the internet to use zoom, or have a preference for a telephone conversation. Telephone interviews will use the same semi structured format as zoom interviews. They will be conducted by either a HWL team member or more experienced volunteer who is able to simultaneously make notes of the discussion.
3.4.3 Self complete on line questionnaire
This has been designed in order to reach a potentially wider number of participants and also support some triangulation of results. This will be widely publicised through a number of specialist and more mainstream on line channels. For individuals who wish to respond but, prefer a paper copy, this option will be available on request.
3.4.4 Focus groups via zoom
We plan to use focus groups through zoom webinars to help gain a greater understanding of some key themes and ideas of young people themselves. These will be held at key stages of the research, during the analysis stage to help interpret initial findings and themes. We also anticipate using this method to help frame recommendations for change and improvement.
As our three target groups of participants are quite diverse, this will be a key consideration in how we frame different focus groups. Our thinking at present is that there will be separate sessions around complex needs and we would aim to run these jointly with Family Action. Similarly we would aim to collaborate with both Mosaic and the Well Centre around hosting sessions involving people in our other groups.
The number, dates and format are to be devised, led by the progress on the research and will be widely publicised.
3.5 Talking to people who work with those in transition
While the primary focus of the research is to discover young people’s experiences, views and ideas, we also want to get some insights from staff who work on transition about what the issues are from their perspectives and any ideas for change they might have. To achieve this we will be holding a webinar in mid October 2020 involving CAMHS, AMHS and SEN services.
3.6 Publicising and inviting participation
Publicity to recruit participants will be based on the characteristics at 3.3 above to enable individuals to self-identify whether they fit the criteria.
Focused promotion
We will negotiate with services who hold the contact details of individuals who might meet the criteria for participation with a view for them to make contact on our behalf using HWL material. A link to the self complete questionnaire will also be sent to out to these groups. Key stakeholders are:
- Well Centre; promoted through direct email / mail to people on the database who meet the age criteria.
- CAMHS; promoted through direct email / mail to people who are open cases (aged 15-18 yrs) or cases which have been closed following transition where the person would now be 21+yrs.
- Mosaic; promoted through the young adults group to people who meet the age criteria.
- SEN service; direct email / mail to a sub set (to be agreed with the service) of young people with EHCPs who are open cases – and where appropriate, where cases have been closed over the previous 12 months following ‘transition’.
- Family Action; promoting through the mailing list to parents of children who meet age and SEN (to be agreed) criteria.
- KAOS at KCH; promotion through contact list of the service for people who meet the age criteria who are Lambeth residents.
- Khulisa; promotion through newsletter and website.
- Kooth; promotion through newsletter and website.
- Rathbone, promotion through newsletter and website.
General promotion
In addition to focused promotion of the research we will also publicise it through more general channels. In each case an invitation to participate in an individual interview and link to the self complete on line questionnaire will be included.
- Lambeth Made webpages , tweets and Facebook
- HWL webpages and email list, tweets and Facebook
- Black Thrive webpages and email list, tweets and Facebook
- Carers Hub webpages, email contact lists.
4. Collaboration and ownership
4.1 HWL is committed to the principles of involvement and will actively seek opportunities to engage all stakeholders in the design, delivery and framing the results of the research. We would like young people (and their parent/carers) to be an ongoing reference point at key stages in the research and to help to shape the outputs and recommendations. To achieve this we aim to use reference groups of young people including those at Mosaic Clubhouse, the Well Centre and CAMHs. It is anticipated that reference groups will be conducted virtually on line at this point and form an integral part of the methodology of the research.
4.2 It is important that the research be ‘owned’ across Lambeth Together as a whole, as it cuts across the Neighbourhoods, Living Well Network and Lambeth Made alliances – this is in expectation that the findings and recommendations will require integrated, jointly owned solutions across the whole of the borough to achieve positive experiences and outcomes of young people with mental health needs transitioning to adult life.
5. Outputs and outcomes
We expect the outputs from the research to provide insights into how the experience of transition to adult life can be improved to help achieve and sustain mental wellbeing for this group.
Recommendations will cover how commissioning could be undertaken differently; how the individual transition journey between services (statutory, young people’s to adults, and third sector) and also how wider services and community resources could be used more effectively, including for example, social prescribing through the PCNs.
To accompany the recommendations we will develop and publish an outcomes framework. Our aim is to actively collaborate with commissioners and key services to understand the impact of their responses to our recommendations on the experiences of young people in transition, following up after 6 months and a year after the completion of the research.